Lets explore the hypertension nursing notes
Hypertension definition
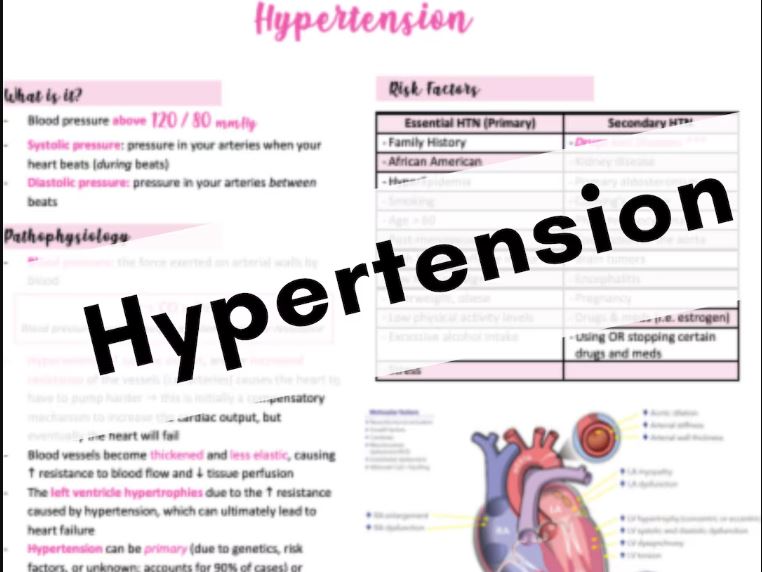
Blood pressure is defined as the pressure or force exerted against the walls of the vessels in which it is contained. High blood pressure, known as hypertension, can result from a change in cardiac output, a change in peripheral resistance, or both.
Blood pressure readings are measured always in millimeters of mercury (mmHg) and are usually given as two numbers.
- The top number is systolic pressure
- considered high if it is over 140 most of the time
- It is considered normal if it is below 120 most of the time.
The bottom number is the diastolic pressure
- It is considered high if it is over 90 most of the time
- It is considered normal if it is below 80 most of the time
It is a systolic blood pressure greater than 140 mm of Hg and a diastolic pressure greater than 90 mm of Hg over a sustained period, based on the average of two or more blood pressure measurements taken in two or more contacts with the health care provider after an initial screening.

Classification of Blood Pressure for Adults age 18 and older
| Category | Systolic (mm Hg) | Diastolic (mm Hg) |
| Optimal | < 120 | < 80 |
| Normal | <130 | <85 |
| High – normal | 130 – 139 | 85 – 89 |
| Hypertension Stage 1 Stage 2 Stage 3 | 140 – 159 160 -179 > 180 | 90 – 99 100 – 109 >110 |
Causes of hypertension
- Though the exact causes of hypertension are usually unknown, there are several factors that have been highly associated with the condition. These include:
- Smoking
- Obesity
- Diabetes
- Sedentary lifestyle
- Lack of physical activity
- High level of salt intake
- High levels of alcohol consumption
- Stress
- Aging
- Genetics and a family history of hypertension
Types of hypertension
- Primary hypertension
– Also known as essential/idiopathic hypertension. It is the most common form of hypertension, accounting for 90 – 95% of all cases of hypertension. It is defined as high BP with no apparent cause. However, there are a number of factors associated and HTN development: genetics, diet, weight and lifestyle.
- Secondary hypertension
– It accounts for 5 – 10% of all cases of HTN, which is defined as high BP caused by pre-existing physical conditions such as kidney disease, thyroid condition, diabetes, etc.
- White coat hypertension
– It is defined as HTN in people who are normotensive except when their BP is measured by a health professional.
- Isolated systolic HTN
- It occurs when the systolic BP is 140 or higher but the diastolic BP remains less than 90 mm of Hg. It is thought to emerge because of increased cardiac output or atherosclerosis–induced changes in blood vessel compliance or both in older adults.
- Malignant HTN:
– It is a syndrome of markedly elevated BP above 140 mm of Hg associated with papilledema
- Benign HTN:
– Also known as uncomplicated HTN, usually of long duration and mild to moderate severity may be primary or secondary
Pathophysiology of hypertension
Due to various causes
Kidney release Renin
Renin helps convert Angiotensin to Angiotensin I in the liver
Angiotensin I is converted into Angiotensin II in the lungs
Angiotensin II causes arterial constriction and Aldosterone secretion in the kidney
Aldosterone causes sodium and water to be retained in the system
Retained sodium and water increase blood volume
Increased blood volume causes arterial constriction which increases peripheral vascular resistance
Increased blood volume and vascular resistance
Hypertension
Hypertension Clinical Features
- Usually asymptomatic until it becomes severe. Extremely high BP may lead to some symptoms and these include:
- Severe headaches
- Fatigue or confusion
- Dizziness
- Nausea
- Problem with vision
- Palpitation, excessive perspiration
- Spontaneous nose bleeding
- Irregular heartbeat
Diagnosis for HTN
- History and physical assessment: Initial assessment of the hypertensive people should include a complete history and physical examination
- Monitoring BP
- Blood test:
- Serum creatinine is measured is measured to assess for the presence of kidney disease, which can be either the cause or the adult of hypertension.
- Urine test:
- Additionally, testing of urine samples for protein is used as a secondary indicator of kidney disease.
- ECG
- A chest X-ray may also be performed to look for signs of heart enlargement or damage to the heart
Prevention
- Lifestyle changes are recommended to lower blood pressure, before starting drug therapy.
- Maintain normal body weight for adults
- Reduce dietary sodium intake
- Engage in regular aerobic physical activity such as brisk walking
- Limit alcohol consumption
- Consume a diet rich in fruit and vegetables.
Management on HTN
- Lifestyle modifications
- The first-line treatment for hypertension is identical to the recommended preventive lifestyle changes and includes dietary changes, physical exercise, and weight loss. These have all been shown to significantly reduce blood pressure in people with hypertension.
- If hypertension is high enough to justify immediate use of medications, lifestyle changes are still recommended in conjunction with medication
- Different programs aimed to reduce psychological stress such as biofeedback, relaxation, or meditation are advertised to reduce hypertension.
2. Medications
– Either diuretics or beta blockers for non-complicated HTN in low dose, is used if not fall BP than 140/ 90 the dose is increased
- If BP is less than 140/90 for a year, a gradual reduction in type and dose of medicine is done
- ACE inhibitors: Blocks formulation of angiotensin II and promote vasodilatation
- Diuretics: Liberation of aldosterone and eliminate of sodium and water in urine
- Calcium channel blocker: Relaxes smooth muscles in the arterial walls, causes vasodilation
- The Cochrane collaboration, World Health Organization and the United States guidelines supports low dose thiazide based diuretic as first line treatment. The UK guidelines emphasize calcium channel blocker in preference for people over age of 55 years or if of African or Caribbean family origin, with angiotensin converting enzyme inhibitors (ACE- I) used first line for younger people
Nursing Management of Hypertension
- History taking
- Physical examination: Auscultate heart rate and palpate peripheral pulses; determine respiration
- Look for edema, spasm, and hemorrhage of the eye vessels.
- Examine the heart
- Determine mental status
- Determine blood pressure.
Nursing Diagnosis
- Acute pain related to increased cerebral vascular pressure
- Ineffective tissue perfusion related to impaired circulation
- Activity intolerance related to imbalance between oxygen supply and demand
- Knowledge deficit related to lack of information about the disease process and self care
- Risk for decreased cardiac output related vasoconstriction
Intervention
- Acute pain related to increased cerebral vascular pressure
- Note the clients attitude toward pain
- Determine intensity(using pain scale) and location of pain, onset and duration
- Encourage and maintain bed rest during acute phase
- Provide non pharmacological measures to reduce pain
- Administer medicine as prescribed.
- Ineffective tissue perfusion related to impaired circulation
- Maintain bed rest, elevate the head position in bed patients.
- Measure input and output
- Observe the sudden hypotension
- Ambulation within tolerance or as advised and avoid fatigue in patients
- Maintain fluids and medications according to medical advice
- Activity intolerance related to imbalance between oxygen supply and demand
- Instruct patient in energy conserving techniques
- Allow patient for bed rest
- Encourage progressive activity and self care when tolerated
- Knowledge deficit related to lack of information about the disease process and self care
- Describe the nature of the disease and the purpose of the procedure and the treatment of hypertension
- Explain the importance of a peaceful environment and therapeutic, and management of stressors
- Discuss the importance of maintaining a stable weight
- Explain to maintain proper fluid intake, amount allowed, and restrictions such as caffeinated coffee, tea and alcohol
- Explain every procedure before performing
- Risk for decreased cardiac output related vasoconstriction
- Provide calm, restful surroundings, minimize environmental activity and noise.
- Maintain activity restrictions; schedule uninterrupted rest periods; assist patient with self–care activities as needed
- Provide comfort measures
- Instruct in relaxation techniques, guided imagery, distractions
- Monitor response to medications to control blood pressure
Leave a Reply