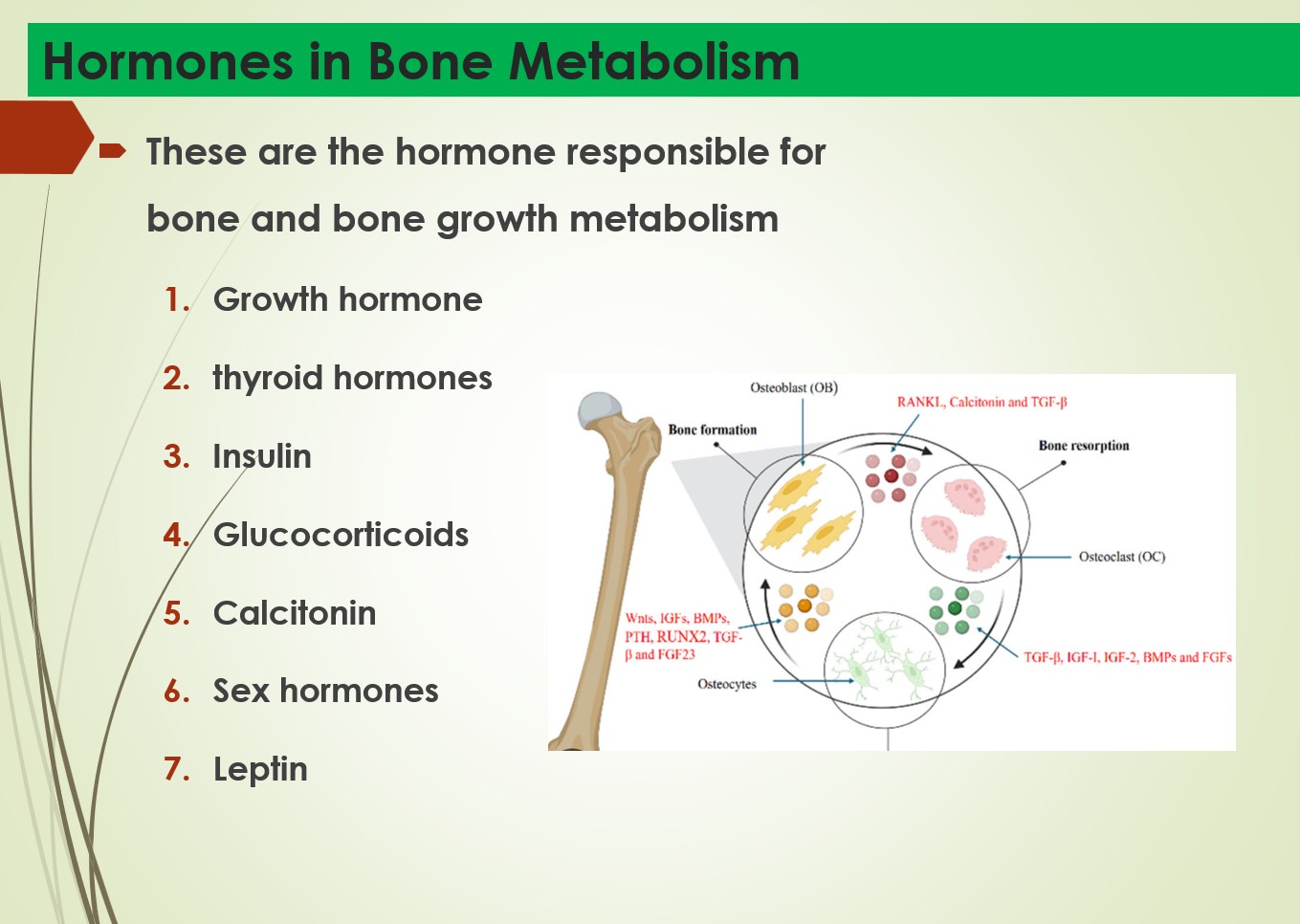
These are the 7 hormones responsible for bone and bone growth metabolism
- Growth hormone
- thyroid hormones
- Insulin
- Glucocorticoids
- Calcitonin
- Sex hormones
- Leptin
Growth Hormone (GH)
Action:
- • Stimulates IGF-1 (somatomedin) from liver
- • IGF-1 → chondrocyte proliferation in epiphyseal plate
- • Longitudinal bone growth
- :
Clinical Correlation
- Excess pre-fusion → Gigantism
- Excess post-fusion → Acromegaly
- Deficiency → Dwarfism (proportionate)
Parathyroid Hormone (PTH)
- Action:
- • ↑ Osteoclast activity → bone resorption → ↑ serum Ca²⁺• ↑ Renal Ca²⁺ reabsorption
- • ↑ Vitamin D activation (1α hydroxylase)
- Clinical Correlation:
- • Hyperparathyroidism → Osteitis fibrosa cystica• (Brown tumours, pathological fractures, ‘pepper-pot skull’) Hormones in Bone Metabolism
- Calcitonin Action:
Calcitonin
Action:
- Secreted by parafollicular C-cells of thyroid
- ↓ Osteoclast activity → ↓ bone resorption → ↓ serum Ca²⁺
Therapeutic use:
- Paget’s disease, oasteoporosis, hypercalcaemia
- •Calcitonin nasal spray used in post-menopausal osteoporosis
Sex Hormones (Oestrogen / Testosterone)
Action:
- ↑ Osteoblast activity; inhibit osteoclasts
- Cause epiphyseal plate fusion at puberty
- Maintain bone density throughout reproductive life
Clinical:
- Oestrogen ↓ (post-menopause) → post-menopausal osteoporosis
- Most common cause of osteoporosis worldwide
Thyroid Hormones (T3/T4)
Action:
- required for normal bone development and maturation
- Stimulate osteoblast activity and collagen synthesis
- Permissive for GH action on the growth plate
Clinical Correlation:
- Hypothyroidism → delayed bone maturation, cretinism, short stature
- Hyperthyroidism → accelerated bone resorption, osteoporosis
Glucocorticoids (Cortisol)
Action:
• Inhibit osteoblasts → ↓ bone formation
• ↓ Intestinal Ca²⁺ absorption
• ↑ Renal Ca²⁺ excretion → 2° hyperparathyroidism
ClinicalCorrelation
• Prolonged exogenous steroid use → glucocorticoid-induced osteoporosis
• Most common preventable cause of secondary osteoporosis
Insulin
Action:
- Stimulates osteoblast activity and bone formation
- Promotes collagen synthesis in bone matrix
- Increases amino acid uptake by osteoblasts
Clinical Correlation:
- Type 1 DM (insulin deficiency) → reduced bone density
- Osteoporosis risk increased in poorly controlled diabetes
Leptin (from adipocytes)
Action:
- Acts via the hypothalamus to regulate bone remodelling• Central pathway: ↑ SNS activity → ↓ osteoblasts
- Peripheral (direct): ↑ osteoblast proliferation
Clinical Correlation:
- • Obesity paradox: high BMI is protective against osteoporosis
- • Leptin deficiency (ob/ob mice) → high bone density
Leave a Reply